
The Silence is Not Health: The Structural Cost of Moralised Pain
Why Coerced Acceptance in Chronic Pain Care Breeds Resignation not Recovery

I. Executive Summary
I would like to present theoretical and empirical synthesis concerning the systemic failure of modern pain management. It argues that chronic physical pain is a biological fact that cannot be thought away through cognitive reframing. By utilising a framework of Regulation Architecture, I demonstrate how current medical demands for acceptance force subjects into a state of resignation and learned helplessness. This silence is not health. It is a trauma response that masks a total collapse of structural integrity. By integrating neuroimaging data and allostatic load theory, this paper calls for a shift from policing emotional reactions to providing functional, biologically grounded relief.
For high-endurance individuals, coerced acceptance does not reduce distress. It interacts with pre-existing regulatory structures that escalate effort under criticism. The result is not peace but intensified containment. What appears externally as improvement may in fact be the strengthening of suppression mechanisms within an already metabolically taxed system.
---
II. Core Definitions: The Architecture of Regulation
To understand the failure of current interventions, we must first define the internal systems of the human animal. Regulation Architecture refers to the underlying biological and psychological system that manages an individual’s energy, output, and response to threat.
Within this architecture sits the Internal Auditor. This is a cognitive and regulatory mechanism that monitors the self for performance and compliance. In high endurance individuals, the Auditor becomes a hyper developed enforcer of composure. It ensures that the structure appears stable even when it is carrying a load far beyond its capacity. This mechanism explains why patients can perform health and appear calm while their nervous system is in a state of high alert.
The Internal Auditor operates through an optimisation–enforcement loop. It detects deviation from internal or external standards, escalates corrective effort, and applies internal pressure until the perceived gap is reduced. What varies between individuals is not the presence of the Auditor but its calibration. Calibration determines how quickly “not enough” is triggered, how intensely effort escalates, and whether performance becomes fused with personal worth. Calibration is shaped developmentally and socially through parental feedback, institutional reinforcement, professional environments, and cultural narratives that equate effort with virtue.
In over-calibrated systems, criticism does not produce withdrawal. It produces escalation. If told to try harder, the structure tightens. If told improvement is insufficient, effort increases automatically. When performance becomes fused with moral worth, failure to improve is experienced not as a technical gap but as a character flaw. In this state, composure is enforced even when the biological system is nearing exhaustion.
---
III. The Biological Receipt: Empirical Evidence for the Internal Auditor
The Internal Auditor is not a metaphor; it is a functional neurological circuit. Its existence is evidenced by the "Biological Receipt"—the measurable physiological cost of maintaining composure under duress. To ground the Auditor in known science, we look to four specific markers:
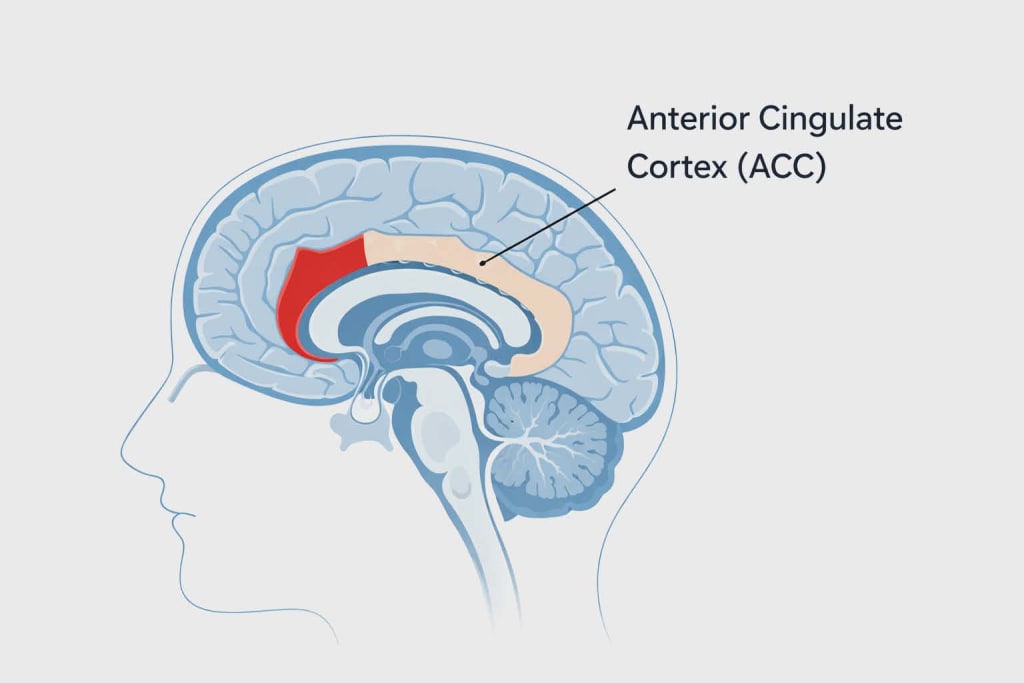
1. The Anterior Cingulate Cortex (ACC) as Hardware
The ACC functions as the brain’s "Conflict Monitor." It is the physical region that detects the gap between an internal state (pain) and an external requirement (acceptance/composure). When the ACC detects this discrepancy, it triggers the Prefrontal Cortex to "fix" the behavior. This is the Auditor’s engine; it generates the "not enough" signal that drives high-endurance individuals to escalate their effort.
2. The Metabolic Cost: The "Glucose Drain"
High-effort suppression is one of the most metabolically expensive tasks the brain can perform. We can prove the Auditor’s work by measuring "Executive Fatigue." When a patient is hyper-focused on "performing health," they lose the capacity for other cognitive tasks. This is not a lack of willpower, but a literal theft of fuel; the Internal Auditor consumes the system’s ATP and glucose to maintain the mask of stability.
3. The Discrepancy in the "Silent" fMRI
As noted by Wager et al. (2013), the Neurologic Pain Signature (NPS) can remain active at high intensities even when a subject reports "feeling fine" due to cognitive modulation. The Internal Auditor acts as the "filter" between the Biological Signal (the scream) and the Social Output (the silence). The presence of a 10/10 biological signal alongside a 0/10 behavioral report is the empirical proof of the Auditor’s containment field in action.
4. Allostatic Load and Stress Hormones
If "acceptance" were a biological cure, stress markers like cortisol would decrease. However, in cases of coerced silence, cortisol and sympathetic nervous system activity remain elevated. The Auditor enforces behavioral quietude, but it cannot stop the systemic damage. This continued high-stress state leads to the immune compromise and secondary physical collapse predicted by this model.
---
IV. Clarifying the Clinical Trap: Acceptance versus Resignation and Compliance
A fundamental error in modern psychology is the conflation of three distinct states. True acceptance is a volitional state of acknowledging reality without a corresponding loss of agency. However, what is often measured in clinical settings is actually compliance or resignation. Compliance is a performative behaviour where the patient follows the therapist's script to avoid conflict or shame. Resignation is the abandonment of hope for relief under the pressure of medical coercion.
When a patient is told that their only path to virtue is to stop reporting pain, they do not find peace. They find a way to silence the Auditor’s leak. This is a state of quiet collapse rather than recovered function.
For individuals with over-calibrated regulatory systems, therapy can become another performance domain. Improvement becomes a standard to be met. Visible calm becomes evidence of goodness. Under these conditions, the Auditor suppresses distress signals in order to restore moral standing. Behavioural silence is therefore not evidence of neurological quiet but evidence of successful containment.
This dynamic frequently produces a predictable trajectory: prolonged containment, apparent stabilisation, followed by sudden collapse once metabolic limits are exceeded. After collapse, rapid re-containment may occur. The oscillation between collapse and composure is often misinterpreted as emotional instability rather than structural fatigue within an over-controlled system.
---
V. The fMRI Evidence: Functional Reality versus Behavioural Silence
Neuroimaging provides the biological receipt for chronic pain that mindset cannot erase. Researchers such as Wager et al. (2013) have identified a specific Neurologic Pain Signature which remains active regardless of cognitive state. While placebo and expectation can partially modulate this activity in acute experiments, these findings cannot be extrapolated to chronic pain. Most studies on mindset use healthy volunteers subjected to short-term, externally applied heat stimuli. These participants know the pain will stop and they possess intact energy reserves. This is fundamentally different from persistent, internally generated chronic pain which is continuous and unpredictable.
Chronic pain differs structurally from acute laboratory pain in three critical ways. The source is endogenous rather than externally imposed. The duration is continuous and uncertain rather than time-limited. The system processing it is frequently already metabolically taxed rather than operating with intact reserves. Cognitive modulation in laboratory settings occurs from a position of energetic surplus. In chronic pain, suppression is attempted from within depletion.
Chronic pain shifts activity from sensory areas to emotional and cognitive centres as demonstrated by Baliki and Apkarian (2015). This represents a state of metabolic overdrive where the brain burns massive energy to process a continuous threat. Because a patient appears calm, therapists assume the brain is also calm. However, fMRI shows the brain is screaming even when the face remains silent. To ignore this biological load is to ignore the physical reality of the patient’s nervous system.
---
VI. Metabolic Bankruptcy and the Terminal Phase of Exhaustion
A critical but often overlooked clinical marker in chronic pain research is involuntary somnolence and profound lethargy, often mislabelled as fatigue. From a neuroenergetic perspective, this is not a sleep disorder but a structural failure of the regulation system. The persistent processing of nociceptive signals combined with the heavy cognitive load of the Internal Auditor creates a state of metabolic bankruptcy.
When the prefrontal cortex is in a state of executive overdrive, the demand for ATP and glucose becomes unsustainable. Involuntary sleep and total system exhaustion represent the brain’s protective mechanism to prevent neurochemical collapse. It is the biological equivalent of a circuit breaker flipping when the electrical load exceeds its capacity. For the researcher, observing these shutdown states provides empirical evidence that the subject is operating at the absolute limit of their allostatic capacity.
Over-controlled individuals may maintain containment for extended periods before collapse. The pattern is not chaotic instability but prolonged plateau followed by sudden decompensation. After collapse, rapid re-containment may occur if environmental pressure remains high.
To mislabel this exhaustion as depression or simple fatigue is a category error.
---
VII. The Duration Fallacy and the Metabolic Bill
A major flaw in current therapy is using outliers such as monks or athletes to argue that pain is a choice. This is a scientific error of scale. Outliers manage volitional pain with a known off switch. Chronic pain is twenty-four hours a day and involuntary. High-effort suppression is a depleting resource. Chronic patients operate with a near-empty tank because the pain has already stolen their energy and concentration. Demanding high effort suppression from a depleted system is an acceleration of systemic failure.
For individuals with over-calibrated audit systems, such demands do not produce defiance. They produce intensified effort.
---
VIII. The Social Architecture of Shame and Epistemic Injustice
When physical pain does not stop, the system often takes away the voice of the patient through guilt and shame. By framing acceptance as a moral achievement, any continued report of agony is treated as a character flaw. This is a form of epistemic injustice, a concept explored by Miranda Fricker, where a patient’s sensory reality is unfairly ignored or pathologised.
High-control clinicians and institutions may inadvertently reinforce this mechanism if their own regulatory calibration mirrors the containment style they reward. Excess composure becomes normalised because it resembles the regulatory style of those assessing it. This positional blindness allows resignation to be misinterpreted as resilience.
The Internal Auditor uses shame to enforce a mask of competence because the social cost of speaking has become higher than the cost of the agony itself. This is not a clinical success but a psychological gag order that removes the alarm while leaving the biological fire burning.
---
IX. The Pedigree of an Error and the Metrics of Failure
The medical community adopted acceptance as a gold standard for economic reasons. Psychological interventions are cheaper than long-term medical relief. Meta-analyses of Acceptance and Commitment Therapy (ACT) and Cognitive Behavioural Therapy (CBT) for chronic pain typically show only a zero point five drop on a ten-point scale. This is statistically significant for research but clinically meaningless for a patient in agony. The system has rewarded quiet compliance over biological relief, treating the silence of the patient as evidence of the success of the therapy.
Long-term follow-up frequently demonstrates attenuation of pain relief even when psychological flexibility scores remain stable. Therapy may succeed in increasing reported acceptance while failing to materially reduce biological load. After repeated invalidation, some patients disengage not impulsively but tactically, recognising that continued reporting increases shame without increasing relief.
---
X. Reconceptualising Catastrophising as Adaptive Monitoring
Psychological frameworks often label attention to pain as catastrophising. This construct fails to account for the realities of chronic pain. Thinking about unavoidable daily pain is adaptive monitoring rather than rumination. Feeling the need for help when a condition cannot be self-resolved is rational and regulatory. Regulatory emotions such as anger and frustration are functional signals that communicate boundary violations. Suppressing these signals removed critical feedback and contributes to functional collapse.
---
XI. Long-Term Outcomes: Allostatic Collapse and Redirection
If silence were healing, life would expand. Instead, patients maintain a mask of competence while their life-space constricts. The biological bill known as allostatic load continues to mount. This wear and tear leads to immune compromise and secondary physical collapse. We must move toward biologically integrative pain models and rights-based care models. These frameworks should validate ongoing biological realities and preserve regulatory emotions rather than policing them.
---
XII. Conclusion: The Required Shift
The refusal to leak the weight of pain does not make it disappear. A structure can only hold an unvented load for so long before it fails. True health requires functional relief rather than policing emotional responses. We must stop treating patient silence as a clinical goal. The structural cost of moralised pain is clear. Without recognition of persistent and uncontrollable biological stressors, interventions risk creating quiet resignation rather than recovery.
---
References
Apkarian, A. V., and Baliki, M. N. (2015). The Vicious Cycle of Chronic Pain: A Neurobiological Perspective.
Fricker, M. (2007). Epistemic Injustice: Power and the Ethics of Knowing.
Sterling, P., and Eyer, J. (1988). Allostasis: A New Paradigm to Explain Cost-of-Regulation.
Wager, T. D., et al. (2013). An fMRI-Based Neurologic Signature of Physical Pain. New England Journal of Medicine.
About the Creator
Keep reading
More stories from Claire McAllen and writers in Humans and other communities.
At My Wits’ End
Life is about taking out the trash and calling it trash because you have every reason to. It wasn't meant to be linear, they say. But the times you tried to make it straight led to problems, and you didn’t have the tools to put any of it to use. You don't put your right shoes on the right feet; you put the left shoes on the left feet. The grey hardened slab will trip you up anyway.
By Caitlin Charlton3 days ago in Humans
Smooth Error
The Pulse Mara learned to read the city the way her grandmother read weather: by the way light pooled on the sidewalks, by the cadence of footsteps, by the hush that fell when the trams slowed. Then the Pulse arrived — a single, humming system that promised to make everything efficient. It listened to traffic, to power grids, to hospital wait times, to the number of empty chairs in cafés. It promised fewer shortages, faster commutes, cleaner air. It promised that the city would finally behave like a well-tuned instrument.
By Kristen Barenthaler5 days ago in Humans




Comments
There are no comments for this story
Be the first to respond and start the conversation.